Quick Answer: Who Is This Program For?
A second opinion TMJ treatment Arkansas patients trust starts with a complete diagnostic workup — not guesswork. My Second Opinion and Complex Case Program is for patients who have already tried something — and it has not worked.
If you have been dismissed, given a night guard that made things worse, told surgery is your only option, or failed CPAP and were sent home without an alternative, this program exists for you. What makes it different is the depth of the diagnostic workup: I use technology and clinical methods that most general dentists and many specialists do not have in-office, and I review everything your prior providers found alongside what I find. You leave with a written diagnosis and a clear path forward — not more uncertainty. CPAP intolerance is a recognized clinical challenge; the American Academy of Sleep Medicine supports oral appliance therapy as a primary alternative for appropriate patients.
Who Needs a Second Opinion for TMJ Treatment in Arkansas
You do not need to have a perfect file or a clear diagnosis to come see me. In fact, most of the patients who benefit most from this program arrive without one. You may be the right fit if:
- A previous provider told you your TMJ pain was “not that bad” or that nothing was structurally wrong, but you know something is not right.
- You were given a night guard — either over-the-counter or custom — and your symptoms either did not improve or got worse.
- You have been told that jaw surgery or joint replacement is your only remaining option, and you want to know whether conservative treatment has genuinely been exhausted first.
- You were diagnosed with obstructive sleep apnea, prescribed CPAP, and could not tolerate it — and your provider did not offer an alternative.
- You have seen multiple providers across dental and medical specialties and received conflicting diagnoses or no clear diagnosis at all.
- You have complex, layered symptoms — jaw pain, headaches, neck tension, poor sleep, ear symptoms — that no one has addressed as a connected system.
These are not unusual presentations. They are the majority of what I see.
What the Two-Hour Diagnostic Workup Finds That Prior Providers Missed
Most TMD evaluations in general dental practice take fifteen to twenty minutes. Mine takes two hours — and that is not a marketing point, it is a clinical necessity. According to the National Institute of Dental and Craniofacial Research, TMJ disorders are complex and often require thorough diagnostic assessment.
Here is what we do and why it matters:
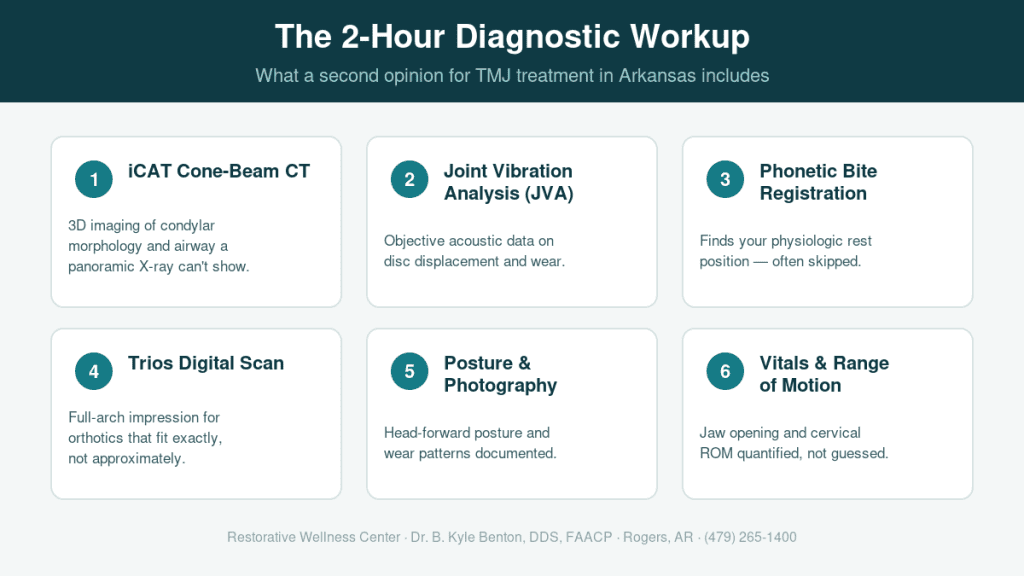
iCAT Cone-Beam CT (CBCT). A panoramic X-ray cannot show condylar morphology in three dimensions. An iCAT CBCT can. I routinely find joint degeneration, condylar asymmetry, and airway anatomy that prior imaging missed entirely because the imaging was not sufficient for the question being asked.
Joint Vibration Analysis (JVA). JVA captures the acoustic signature of your joints in motion — disc displacement, adhesions, and degenerative changes produce vibration patterns that are measurable and documentable. This is objective data, not a clinical impression.
Phonetic Bite Registration. Establishing where your jaw naturally wants to close — your physiologic rest position — is foundational to any orthotic treatment. Many prior providers skip this step and build appliances to an acquired bite that is itself a compensation pattern.
Trios Digital Scan. A full-arch digital impression gives me the precision to fabricate orthotics that fit exactly rather than approximate.
Posture and Intraoral Photography. The jaw does not exist in isolation. Head-forward posture, cervical muscle tension, and occlusal wear patterns are part of the same picture, and I document all of them.
Vital Signs and Range-of-Motion Assessment. Restricted jaw opening, lateral deviation, and cervical range of motion are quantified, not estimated.
At the end of the two-hour workup, you receive a written treatment plan — a real document with findings, diagnosis, and recommended treatment options. You can take it home, review it, and decide without pressure.
Surgery as a Last Resort, Not a First Answer
I am a conservative, non-surgical provider. That is not a limitation — it is a deliberate clinical position.
Surgery for TMD carries real risks and, in many cases, is pursued before conservative options have been genuinely tried. Stabilization orthotics using the Olmos SSC protocol, phonetic bite registration, photobiomodulation, and PRF are legitimate interventions that can produce significant improvement in pain and function without irreversible structural intervention.
If you have been told surgery is necessary, I want to look at your imaging, review your records, and give you an honest second opinion. Sometimes surgery is appropriate. But in my experience, it is far less often the right first step than patients have been led to believe.
How I Use Your Prior Records
I ask every second opinion patient to bring whatever they have — not because I want to critique prior providers, but because your records tell me what has already been tried and what has not.
Prior imaging, prior appliances, prior diagnoses, and prior treatment timelines are all clinically useful. They help me understand why previous treatment did not work and what approach is most likely to work now. You do not need a referral and you do not need a complete file. Bring what you have.
What to Bring to Your Evaluation
- Any prior imaging: panoramic X-rays, MRI, CT scans
- Prior appliances (night guards, splints, oral devices) — even if you stopped wearing them
- A list of providers you have seen and treatments you have tried
- Any written diagnoses or treatment plans you have received
- Your current medication list
- Sleep study results if applicable (home sleep test or polysomnography)
- Insurance cards for medical and dental coverage
If you do not have any of these things, come anyway. The evaluation stands on its own.
Frequently Asked Questions
Do I need a referral for a second opinion at Restorative Wellness Center?
No referral is required. You can contact us directly to schedule your evaluation. We welcome patients who are coming on their own initiative, and we are experienced at working with patients whose prior care was managed elsewhere.
What if my prior provider says surgery is the only option — is it too late for conservative treatment?
Not necessarily. Whether conservative treatment is still viable depends on what your joints look like now — and the only way to answer that is with current, high-quality imaging and a thorough clinical exam. I have seen patients told surgery was their only path who responded well to stabilization orthotics. I have also seen patients for whom surgery was genuinely indicated. I will give you my honest assessment either way.
I failed CPAP. Can oral appliance therapy help me?
OAT is a recognized alternative for patients with mild to moderate obstructive sleep apnea who are CPAP-intolerant. For moderate to severe cases, I work in coordination with your physician or sleep medicine provider. If you have a sleep study, bring it — it tells me what severity range we are working with and whether OAT is the appropriate first-line intervention.
How is your diagnostic approach different from what I have already had done?
The difference is primarily in the technology and the time. A two-hour evaluation using CBCT, JVA, digital scanning, and phonetic bite registration gives me a dimensional picture of your joints, your airway, and your bite that a standard dental exam cannot produce. That picture is what allows me to make a diagnosis that holds up — and to recommend treatment with confidence rather than guesswork.
You Deserve a Clear Answer
If you have been living with pain, poor sleep, or unresolved jaw symptoms — and prior care has not given you a path forward — I want to see what we can find together. Why patients choose us for complex cases comes down to one thing: we do not guess and we do not rush.
You can read more about Dr. Benton’s credentials and training if you want to know the clinical background behind this approach.
When you are ready, request your second opinion evaluation. The two hours you spend in our office will give you more clinical clarity than most patients have had in years of treatment.
Restorative Wellness Center
Dr. B. Kyle Benton, DDS, FAACP
2603 W Pleasant Grove Rd, Suite 111 | Rogers, AR 72758
(479) 265-1400 | restorativewellnessar.com
Serving Rogers, Bentonville, Fayetteville, Springdale, Siloam Springs, Fort Smith, and Northwest Arkansas